If you’ve been living with unpredictable cycles, stubborn weight gain, or a fog you can’t quite name — and someone finally mentioned PCOS — you might have felt equal parts relieved and overwhelmed. You’re not imagining it. And no, it’s not just “hormones being hormones.”
Polycystic ovary syndrome (PCOS) is one of the most prevalent yet persistently misunderstood endocrine conditions in women of reproductive age, affecting roughly 1 in 8 women globally. What makes it tricky is that it doesn’t look the same in everyone — and the name itself is misleading. You don’t need polycystic ovaries to have PCOS.
The hormonal web nobody explains clearly
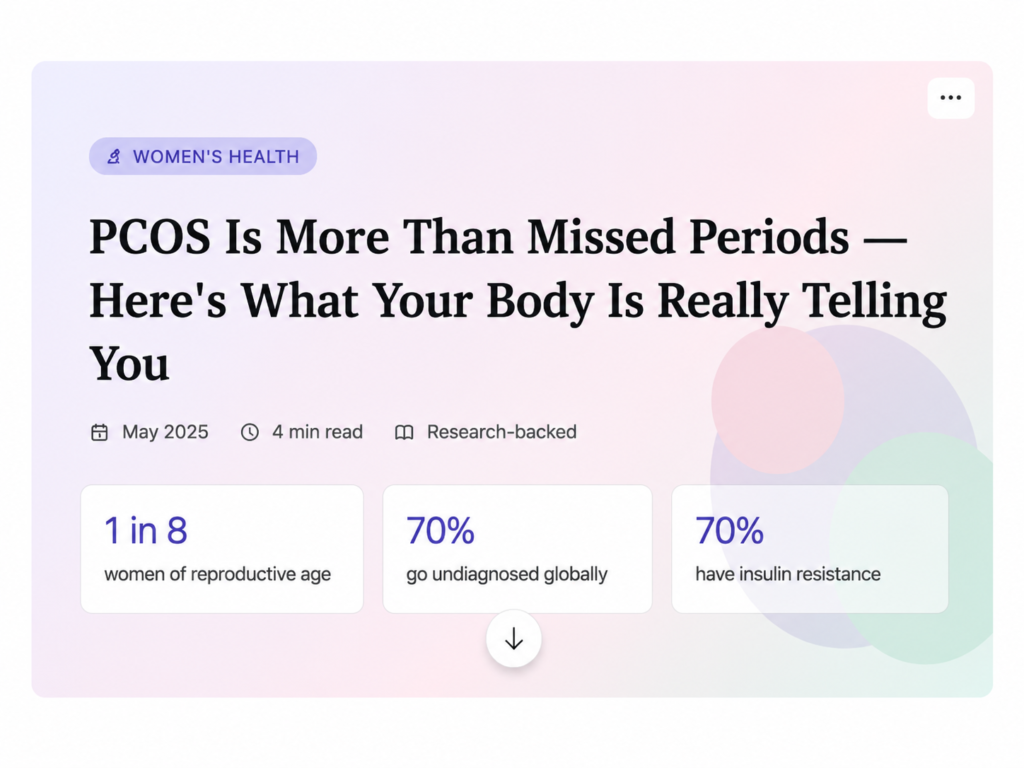
At its root, PCOS is a condition of androgen excess — your ovaries produce more male-type hormones (androgens like testosterone) than they should. This throws off the delicate signaling between your brain, pituitary gland, and ovaries, disrupting the LH/FSH ratio that governs ovulation. But here’s what most articles skip: insulin resistance is present in up to 70% of women with PCOS, and it’s not just a side effect — it’s often a core driver.
Research note: Hyperinsulinemia (chronically elevated insulin) sensitizes the ovary to LH signaling, amplifying androgen production — creating a self-reinforcing hormonal loop that diet and lifestyle alone may not break.
Symptoms that often go unrecognized
Most people know the textbook trio — irregular periods, acne, excess hair growth. But PCOS has a much wider footprint:
The mental health connection is especially underreported. A 2024 bibliometric study found that depression prevalence is significantly higher in women with PCOS than in healthy controls — and the link is biochemical, not just circumstantial. Elevated androgens appear to correlate directly with depressive episodes and impaired stress-coping, independent of obesity or insulin resistance.
Why diagnosis takes so long
Globally, an estimated 70% of women with PCOS remain undiagnosed. Symptoms often debut in adolescence but get dismissed as “normal teenage hormones.” Weight stigma delays investigation. And because PCOS presents differently across body types and ethnicities, lean women with PCOS are particularly likely to fall through the diagnostic net — their metabolic markers look “normal” even when their hormonal profile doesn’t.
Diagnosis today follows the Rotterdam criteria: two out of three — hyperandrogenism, oligo/anovulation, or polycystic ovarian morphology on ultrasound. More recently, anti-Müllerian hormone (AMH) levels are being explored as a replacement marker for ultrasound in the 2023 international guidelines update.
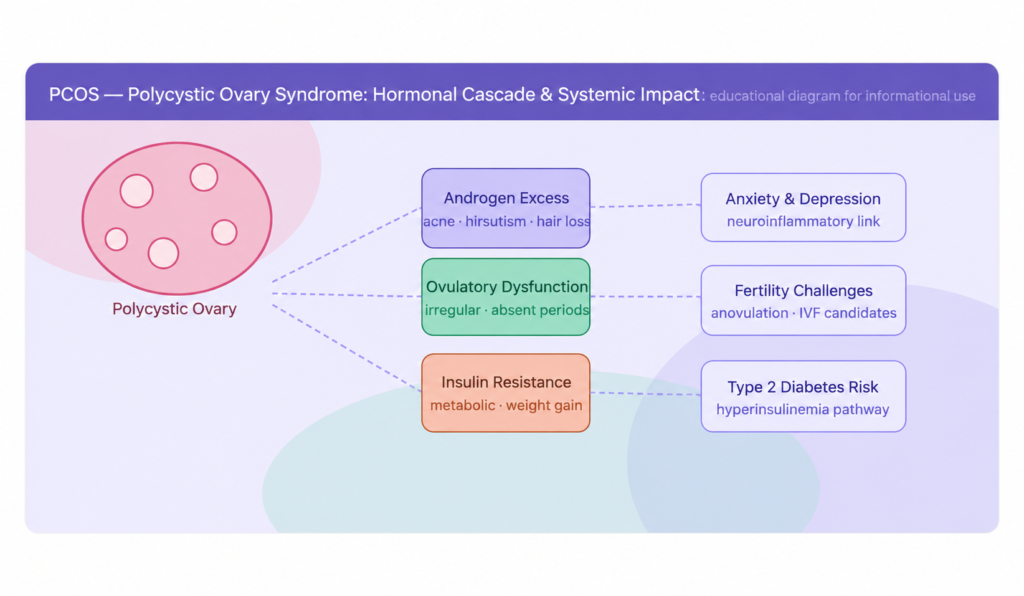
Managing it — beyond the pill
Oral contraceptives are often the first (and only) thing offered. They manage symptoms but don’t address the underlying metabolic dysfunction. If you’re not trying to conceive, that might feel adequate — but it’s worth knowing what else works.
You deserve a fuller picture
PCOS is a chronic, systemic condition — not a “gynae problem” with a tidy fix. It shapes metabolic health, mental wellbeing, fertility, and long-term cardiovascular risk. The goal isn’t to suppress symptoms indefinitely but to understand the root dysfunctions — hormonal, metabolic, inflammatory — and address them with the nuance they deserve.
if something in this resonates, push for a full hormonal panel, a fasting insulin test, and a doctor who listens past the prescription pad. You’re not being dramatic. You’re being thorough.